doi: 10.56294/nds202212
ORIGINAL
Localised chronic fibroedematous gingivitis treated with chamomile-argan oil in patients aged 15-19 years
Gingivitis crónica fibroedematosa localizada tratada con aceite de manzanilla-argán en pacientes entre 15-19 años
Rosa María
Montano-Silva1 ![]() *,
Yoneisy Abraham-Millán1
*,
Yoneisy Abraham-Millán1 ![]() *,
Aliana Peña-Méndez1
*,
Aliana Peña-Méndez1 ![]() *,
Yousemy Álvarez-Romero1
*,
Yousemy Álvarez-Romero1 ![]() *,
Darianna Rubio-Díaz1
*,
Darianna Rubio-Díaz1 ![]() *,
Aliannys González-Alvarez1
*,
Aliannys González-Alvarez1
![]() *
*
1Facultad de Ciencias Médicas Isla de la Juventud. Isla de la Juventud, Cuba.
Cite as: Montano-Silva RM, Abraham-Millán Y, Peña-Méndez A, Álvarez-Romero Y, Rubio-Díaz D, González-Alvarez A. Localised chronic fibroedematous gingivitis treated with chamomile-argan oil in patients aged 15-19 years. Nursing Depths Series. 2022; 1:12. https://doi.org/10.56294/nds202212
Submitted: 07-01-2022 Revised: 19-03-2022 Accepted: 13-05-2022 Published: 14-05-2022
Editor: Dra.
Mileydis Cruz Quevedo
![]()
Corresponding Author: Rosa María Montano-Silva *
ABSTRACT
An experimental study with pre-test, post-test, and a control group was conducted to evaluate the effectiveness of chamomile-argan oil in the treatment of chronic fibroedematous gingivitis in patients at the Martha Machado Cuní Teacher Training Centre between 2020 and 2022. The study population consisted of students aged 15-19 years old at the centre. The population consisted of students diagnosed with some type of gingivitis, and the sample consisted of 68 students diagnosed with localised chronic fibroedematous gingivitis. The aim of this study was to evaluate the effectiveness of chamomile-argan oil in the treatment of localised chronic fibroedematous gingivitis. The variables considered were sex, age groups, presence of chronic fibroedematous gingivitis and effectiveness of chamomile-argan oil. After obtaining informed consent, a thorough interview and clinical examination was carried out on each of the patients who took part in the research in order to achieve the proposed objective. Chronic localised fibroedematous gingivitis was predominant in the population. The study sample was predominantly female, aged between 15 and 16 years, with a diet rich in sugar, poor oral hygiene and hormonal changes as risk factors associated with the onset of gingivitis. Chamomile-argan oil is effective in the treatment of localised chronic fibro-oedematous gingivitis. Taking into account the shortage of medicines in Cuba, the effectiveness of the proposed treatment, and the guidelines established in Cuban state policy, it can be argued that the use of the proposed treatment is highly significant and timely. It would therefore be essential to recommend the production of chamomile-argan oil for the treatment of localised chronic fibro-oedematous gingivitis, as well as for other pathologies affecting the stomatognathic system.
Keywords: Chronic Fibroedematous Gingivitis; Chamomile-Argan Oil; Natural Treatment; Experimental Design; Adolescent Oral Health.
RESUMEN
Se realizó una investigación con diseño experimental con pre-prueba, post-prueba y un grupo de control para evaluar la efectividad del aceite de manzanilla-argán en el tratamiento de la gingivitis crónica fibroedematosa localizada en pacientes del Centro Educacional Formador de Maestros “Martha Machado Cuní”, en el período comprendido entre 2020-2022. El universo de estudio estuvo constituido por los estudiantes del centro entre 15-19 años de edad. La población se conformó con los estudiantes que se diagnosticaron con algún tipo de gingivitis y la muestra fue de 68 diagnosticados con gingivitis crónica fibroedematosa localizada. La presente investigación tuvo como objetivo evaluar la efectividad del aceite de manzanilla-argán en el tratamiento de la gingivitis crónica fibroedematosa localizada. Se tuvieron en cuenta las variables sexo, grupos de edad, presencia de gingivitis crónica fibroedematosa y efectividad del aceite de manzanilla-argán. Previo consentimiento informado se realizó un minucioso interrogatorio y examen clínico a cada uno de los pacientes que formaron parte de la investigación para lograr el objetivo propuesto. Predominó en la población la gingivitis crónica fibroedematosa localizada. En la muestra de estudio predominó el sexo femenino, el grupo de edad entre 15-16 años, así como la ingestión de alimentos ricos en azúcar, higiene bucal deficiente y cambios hormonales como factores de riesgo asociados a la aparición de la gingivitis. El aceite de manzanilla-argán es efectivo en el tratamiento de la gingivitis crónica fibroedematosa localizada. Si se tienen en cuenta el déficit de medicamentos existente en Cuba, la efectividad del tratamiento propuesto, y los lineamientos establecidos en la política del Estado Cubano, se puede alegar que es altamente significativo y oportuno el uso del tratamiento propuesto. Resultaría imprescindible entonces recomendar la producción del aceite de manzanilla-argán para el tratamiento de la gingivitis crónica fibroedematosa localizada, así como para otras patologías que afectan el aparato estomatognático.
Palabras clave: Gingivitis Crónica Fibroedematosa; Aceite de Manzanilla-Argán; Tratamiento Natural; Diseño Experimental; Salud Bucal Adolescente.
INTRODUCTION
Gingivitis is the first stage of periodontal disease, involving inflammation and, in more severe processes, infection, with the possibility of destroying, in some cases, the supporting tissues of the teeth, including the gums, periodontal ligaments, and alveolar bone.(1) The oral health specialist Adolph Witzel (1847-1906) first identified the bacteria that cause periodontal disease. Still, it was not until 1976, in a paper presented by Page and Schroeder, that the pathogenesis of this pathology was first proposed, who defined its histological pattern as an "initial lesion".(2)
It is a frequent and mild form of gum disease, which causes irritation, redness, and inflammation of the part of the gums surrounding the base of the teeth. Chronic gingivitis is the most common protective periodontal disease; its characteristics are similar to inflammation in any other part of the human organism. It usually presents as a single pathological change, primary to the appearance of another process or in addition to other syndromic entities, such as, for example, gingival hyperplasia due to medication or desquamative gingivitis.(1,2)
The leading cause of chronic gingivitis is the microorganisms of the antibacterial plaque. The intimate contact of the organisms that comprise the antibacterial plaque and the subgingival microbiota explains the inflammatory reaction that compromises the gingival epithelium, the underlying connective tissue, and the epithelial adhesion. It is necessary to remember that in this case, the epithelial adhesion does not migrate, i.e., there is a pathological increase in the depth of the gingival sulcus but at the expense of the coronary migration of the margin; therefore, when we speak of chronic gingivitis with pockets, these are: virtual, false, relative or gingival pockets.(3)
Gingival disease is considered the second most common oral disease in terms of morbidity, affecting more than 3 quarters of the population. Gingivitis is an inflammatory process that begins in early childhood, at approximately 5 years of age, with prevalences of 2-34 % in 2-year-olds and 18-38 % in 3-year-olds, which increases as it reaches its peak at puberty.(4,5)
Gingivitis is caused by supragingival plaque deposition. Clinically, it is manifested by reddening the free gingiva and, in part, of the inserted gingiva. In addition, there is variable swelling of the gingiva and the formation of a gingival pocket; however, there is no loss of attachment or bone tissue. The stippling disappears to a greater or lesser extent, and the gingiva bleeds easily when rubbed or after probing the pocket. It is usually a painless and completely reversible pathology whose severity is directly related to accumulated plaque accumulated.(6,7,8)
Gingivitis can occur in children ages 3 to 5 with primary dentition. Its prevalence increases at the onset of puberty and begins to decrease after the age of 14. About 70 to 80 % of children ever suffer from gingivitis. The percentage of adults with gingivitis decreases with age and varies between 35 and 50. Its prevalence is high; about 90 % of individuals worldwide present gingivitis, with a tendency to an exponential increase with age up to 35 years.(9,10)
In Europe, about 50 % of the population is estimated to suffer from this disease. In the Americas, it is remarkable that there are many patients with this disease. International studies have found alarming figures for chronic gingivitis in the school population, showing prevalences above 80 %. Cuba has a high incidence (75 %) and moderate severity.(11,12)
The treatment of gingivitis has evolved over the years; it has been contemplated in medical therapy with drugs or the use of natural medicine. Throughout human development, Natural and Traditional Medicine (NTM) has been used to prevent and cure various pathologies that affect man's health and, therefore, his quality of life.
MNT is considered a medical discipline recognized by the Ministry of Public Health (MINSAP) according to the needs identified by the health services. It is of great importance the knowledge and application of procedures and techniques of health promotion, disease prevention, diagnosis, healing, and rehabilitation that includes this discipline to raise the quality of life, generalizing the use of natural medicines and other therapeutic resources of easy acquisition, low cost and available to all.(13)
In Cuba, the genesis of traditional medicine was practically unknown since the aboriginal population was exterminated at the beginning of colonization and the different ethnic groups that made up the slave population. However, they contributed elements of healing practices and left few testimonies,(14) at the end of the 19th century, there were antecedents of the practice of traditional Chinese medicine in the city of Cárdenas, where the Chinese doctor Chan Bom Biam worked, whose successes were remarkable regarding medicinal plants. The famous phrase "Not even the Chinese doctor can save him" was derived from his work, which pondered the high qualification acquired by the Asian doctor with this therapy.(15)
With the triumph of the Cuban Revolution, the study of MNT began to be encouraged; since the 80s, the National Health System has developed a policy to expand this discipline's knowledge. This medical discipline has different therapies that are called natural, alternative, parallel, or complementary therapies.(16)
Among these therapies is Herbotherapy or Phytotherapy, which is conceived as the branch of medicine that uses phytopharmaceuticals to treat diseases. Phytopharmaceuticals are those preparations from plants(16) that are used for the medicinal therapy of some pathology or its prevention.
Herbal medicine is the oldest form of medical care known to humanity; throughout history, herbs have been used in all world cultures. Nowadays, Herbotherapy or Phytotherapy are the terms used to refer to green medicine, that is, medicine that uses the properties of plants. It is a therapy based on the active principles of plants, which are nothing more than those plant substances that produce a pharmacological effect on the human being; they are found in the place of most excellent metabolic activity of the plant, for example, in the leaves, root, seed or fruit.(4)
Among the pharmaceutical forms of herbal medicines that are most commonly used in stomatology are the following:(17)
· Fluid extracts: are hydroalcoholic preparations of plant drugs, where each milliliter is equivalent to 1 g of the dry drug. They are highly concentrated extracts of the active principles of plants.
· Tinctures: alcoholic or hydroalcoholic solutions prepared with vegetable drugs at comparatively low concentrations.
· Mouthwashes: medicinal liquids for rinsing the oral mucosa.
· Topicals: liquid preparations for local application (also called dabs or dabs).
· Creams: semi-solid preparations, whose base is usually emulsified and sometimes water-soluble, with a soft consistency, which serve as a vehicle for external applications of active principles of plants.
Herbal medicines can also be prepared at home, for a use no longer than 24 hours, in different ways:(18)
· Cooking: whole plant part of it boiled.
· Infusion: freshly boiled water and add plant.
· Macerated: crush and pour boiled water or other liquid.
In case of homemade preparation, certain indications must be taken into account, such as:(18)
· Do not store in metallic containers.
· Do not use for prolonged periods of time.
· Do not mix the plants.
At present, and in contrast to the progress achieved in the creation of new medicines worldwide, natural medicine is gaining more and more advocates and practitioners, mainly due to its natural forms of healing and the lack of side effects. The main problem in achieving greater incorporation of specialized personnel in the practice of the different natural therapies is the lack of a specific orientation that propitiates the minimum indispensable knowledge for their use.
Throughout history, Cuba has applied multiple natural treatments for common ailments. Still, it is necessary for the scientific evaluation of the results obtained in the different therapies, which is essential to incorporate our medical and stomatological personnel into this field. It is not only enough with the use of plants as treatment by the population in general; they must join the action of the population, the army of white coats, with scientifically proven results in the cure of the main pathologies that can cause morbidity and mortality in patients and thus increase their quality of life.
The World Health Organization (WHO) recognizes traditional therapies' importance and global reach. It has even created an Office of Traditional Medicines, noting that they remain largely unregulated in all countries. It is, therefore, necessary for consumers to have information that will enable them to have access to effective, safe, and quality products.(19)
As recognized by the WHO, in primary health care (PHC), up to 80 % of the population in underdeveloped countries relies on traditional medicine. In developed countries, in different proportions and with other philosophies, many people resort to various types of natural remedies because they consider natural to be synonymous with harmless.(20) Developed countries bet on the high and often unnecessary consumption of synthetic drugs, while underdeveloped countries generally use MNT in PHC; not only because of the cost of drugs and the lack of acquisition in the market but also because of the benefits offered by the consumption of natural drugs by the population.
Another reason for hope and depth in the study of plants is the so-called Chinese example, a country that turned around the precarious health situation it found itself in at the end of the Second World War. It fully applied the knowledge of Indigenous traditional medicine (based practically on the integral use of medicinal plants) and simultaneously developed Western medicine. Twenty-one medicinal plants have been used in an industrial process in that nation, starting from an inverse concept to the West.
In Western countries, it is traditional for the protocol followed in developing a new drug to be in the following order: identification of the molecule, experimental pharmacology, and clinical pharmacology. In contrast, in the Chinese experience, it was done the other way around, i.e., starting with proven clinical trials of botanical species and traditional preparations.(21)
The Phytotherapy of tomorrow must approach modernity based on scientific methods, which consider the valid experiences accumulated in the past and which at present require a rational study and understanding on scientifically established bases. Natural medicine will necessarily apply its ideas and protocols for the verification of efficacy and safety, which do not have to be precisely the same as for synthesized compounds.(22)
Logically, both the patient's subjective perception and the physician's more objective perception will have to be considered in the results. If these conditions are met, Phytotherapy can be a continuous stimulus for the pharmaceutical sciences, an essential link in the chain of therapeutic development.
On the contrary, if it remains only as an art based on inherited experience, it will lose its logical development, and with it, Pharmacology, a therapy that, well used and known, can contribute significantly to the growth and health welfare of the population, both in the purely therapeutic and palliative aspect as well as in prevention. Today, therefore, it is an essential goal of therapy with medicinal plants to contribute to establishing the causes of their action and, from here, to establish the relationship between the chemical constituents and their biotherapeutic effects.(22) Another essential aspect is the resistance of various microorganisms to drugs; from this perspective, emphasis should be placed on the continuous challenge faced by drug therapy, most of the time due to their inadequate use. It is then where the confrontation of pathologies through medicinal plants constitutes a key link since adverse reactions and microbial resistance are rare. WHO Guidelines for the use of medicinal plants:(23)
· A correct identification of the plant should be made.
· Never abuse the prolonged use of medicinal plants.
· Their decoctions and infusions should be used in the first 24 hours.
· Fresh or dried plants should be used, but in good condition.
· Do not indicate to pregnant women, especially in the first trimester.
· They should not be extracted from places exposed to chemical products.
· They should not be mixed with other medicines or plants without consulting authorized persons, because they can produce toxicity.
In the 1940s, Dr. Juan Tomás Roig, botanist, pharmacist and agronomist, identified 595 species The Cuban population used these plants for different curative purposes, and in his book Medicinal, Aromatic, and Poisonous Plants of Cuba, he called on the National Scientific Community to study them. The scientist said this would verify their pharmacological activities, pointing out the possibility of developing a pharmaceutical industry from Cuban flora.
In the 1960s, scientific research on medicinal plants began to develop. In the 1970s, the Medicinal Plants Station "Juan Tomás Roig" was inaugurated to initiate the integral study of medicinal plants in Cuba. However, it was not until 1980 that the real work of rescuing traditional medicine began.(24)
The term medicinal plants refers to any plant with active principles that present a pharmacological activity that can be used from a therapeutic point of view. It can be used as a source for extracting the active principles, or the plant can be used directly. Medicinal plants, as the medicines they are, need to be scientifically known by all health professionals who work with them regarding their therapeutic properties and indications. In the same way, the procedures and manipulations they will undergo as raw materials before being used in the elaboration of pharmaceutical preparations should be known.(25) At present, Natural and Traditional Medicine (NTM) is widely applied in the stomatological services of the country, integrating itself favorably to the therapeutic possibilities for the solution of various oral health problems,(26) as well as to the performance of procedures that are part of stomatological treatments. However, sometimes, some difficulties contribute to the fact that it is not applied in every occasion in which it could be indicated.
Since the 1970s, the WHO has promoted the use of NTM modalities that are effective and safe for health care, with the criterion of their integration into national medical systems. In addition, MNT is currently part of the health strategy of the Cuban state since Guideline 158 of the Economic and Social Policy of the Party and the Revolution states that "maximum attention should be paid to the development of MNT ".(27)
With the introduction of MNT in Stomatology, the therapeutic approach to conditions of the oromaxillofacial complex changed. Subsequently, to improve the competence and professional performance of the graduates, MNT was gradually introduced in the undergraduate and graduate curricula of the Stomatology career.
Particular study of Manzanilla:(28)
· Scientific name: Matricaria chamonilla L. The flowers and dried leaves are used.
· Properties: anti-inflammatory, antibacterial, antifungal, antiviral, antiulcer, antiallergic and analgesic.
· Indications: irritations of any kind.
· Distribution: it is native to Europe and Western Asia. It is currently widely distributed worldwide.
· Botanical characteristics: herbaceous plant, cylindrical stem, erect, branched, up to 50 cm high. Chamomile is actually two plants: Roman chamomile (Anthemus nobilis) and German chamomile (Matricaria recutita). Roman chamomile is a low-growing perennial with a slightly stronger fragrance than German chamomile. Both have, like the daisy, flowers that appear toward the end of spring and last until late summer. The branched stem is somewhat erect, round and hollow, and grows to about 20 inches. The leaves are finely divided. The whole plant has a pineapple or apple odor.
· Medicinal properties: as an antiseptic, healing, anti-inflammatory, digestive, diuretic, analgesic, expectorant; used for the treatment of eczema, neuralgia, gastritis and for the disinfection of ulcers and wounds.
· Habitat and distribution: Chamomile is native to the Balkan region, from where it spread to the rest of Europe. Its high level of adaptability has made it naturalized in several regions of the American continent. Its cultivation is mainly for industrial purposes. It develops easily in soil with good drainage and high luminosity. It has good resistance to frost, and tolerates relatively low levels of soil fertility and acidity. It was introduced by the Spanish in Peru in 1928, as an insecticide.
· Chemical composition of chamomile:(29)
· Essential oil (0,3 %-1,5 %): it is the most relevant component, and is obtained from the upper region of the plant. The essential oil is part of the lipophilic group. According to the Argentine Pharmacopoeia, the drug should not contain more than 10 % of fresh plant matter, nor more than 2 % of foreign organic matter. The British Pharmacopoeia requires an essential oil content between 0,25 and 0,70 %.
· The majority of its essence (more than 50 % of the total), expresses the following composition:(30)
a) Azulenes (26-46 %): the main one is chamazulene (6-15 %) and to a lesser extent guajazulene. This is a volatile oil that gives the essence a bluish color. This coloration arises from the action of heat during the extraction process. This is the reason why this characteristic is not expressed in the conventional preparation of its infusion.
b) Sesquiterpenes: it has the following compounds: a-bisabolol (10-25 %) and derivatives (bisaboloxides A, B and C, bisabonlonoxide A).
c) Sesquiterpene lactones: matricarin and deacetylmatricarin. Matricarin is a precursor of chamazulene.
d) Flavonoids (1-3 %): together with mucilages constitute the hydrophilic group of the drug. Numerous flavones and flavonolsmethoxylates have been identified in chamomile, such as apigenin (0,25 to 42 %) and quercetin, with their corresponding glycosides (7 - glucosyl - apigenin and 7-glucosyl quercetin). Also apiin, luteolin, lisorhamnetol, rutin and patuletin, among others, are part of the flavonoids of chamomile.
e) Coumarins: the main coumarins in chamomile are dioxycoumarin, umbelliferone and herniarin.
· Others: in smaller proportions in chamomile we find: valerianic acid; ascorbic acid; angelic acid; salicylic acid; various fatty acids; various tannins; uronic mucilages (10 %); steroids derived from stigmasterol; mucopolysaccharides; bitter principle (anthemic acid), xyloglucurans; mineral salts (8-10 %), triacontane and phytosterin (resins).(31)
· Active principles and properties: these are contained in the chamomile inflorescences, they can be water-soluble or fat-soluble in nature. The liposoluble ones are present in the essential oils.(32) It is characteristic that in chamomile and through oxidative processes, (-)-alpha bisabolol can be found. By means of analogous processes, the (-)-alpha bisabolol enters the plant to form a secondary alcohol called bisabolol oxide.
1. Sulfur glycosides: these are sulfur glycosides. These have antibiotic properties. They require a maceration time of ten minutes in warm water, since only in this way a genin is isolated and becomes active.(32)
Particular study of the Argan tree
Botanical characteristics: it grows to 8-10 meters in height and lives for 150-200 years. And has lived for 150-200 years in the area between Tiznit and Essaouira. It is thorny with a rough trunk. With a rough trunk. It has small leaves of 2-4 cm. It has small leaves 2-4 cm long, oval with a rounded apex. With rounded apex. The flowers are small, with five greenish-yellow petals; they bloom in April. The fruit is 2-4 cm long and 1,5-3 cm wide, with thick skin surrounding the bitter, sweet-smelling shell. The peel surrounds the fruit, which contains 2-3 seeds rich in oil. The fruit takes a year to ripen until June-July of the following year.(33)
The area of Argania forests has decreased by 50 % in the last 100 years due to their use as fuel, grazing, and intensive cultivation. Its best protection for conservation could be found in the recent development of argan oil production for export as a product of high commercial value.(33)
The argan tree (Argania spinosa L., Fam. Sapotaceae) is a unique wild tree in the world that was declared a "Biosphere Reserve" by UNESCO (United Nations Educational, Scientific and Cultural Organization). Its formations constitute a unique agroforestry system, a cultural landscape, and an ethnic and socioeconomic symbol of great value. It is a species of flowering plant belonging to the Sapotaceae family, being native to southwestern Morocco, on the Saharan border, in the semi-desert calcareous lands of the Algerian region of Tindouf (western Algeria), and in the north of Western Sahara (near El Aaiun and Smara).(34)
Argan oil is a virgin oil that is not subjected to a refining process. It has been consumed for centuries in Berber places of origin. The Berber population of the Atlas traditionally uses it as food and as a cosmetic, accounting for up to 25 % of the daily lipid intake in the diet. With tea, argan oil accompanied by honey is offered to guests as a gesture of hospitality in the Souss region. It is now gaining considerable gastronomic, nutritional, therapeutic, and cosmetic interest in other countries and is considered the "gold of the desert ".(33,34)
It is characterized by high levels of linoleic and oleic acid, in addition to being rich in polyphenols and tocopherols, which have important antioxidant activity. The presence of minority compounds such as sterols, carotenoids, xanthophylls, squalene, and CoQ10 also contributes to its nutritional value and antioxidant potential.
Interesting healing and therapeutic properties have been attributed to it since ancient times. Recent studies suggest hypolipidemic, antihypertensive, and hypocholesterolemic effects, as well as the ability to halt the development or progression of some cancers and antiproliferative effects.(35)
At present, the economic blockade is causing major problems, and the health sector has suffered greatly from this injustice. The shortage of medicines to treat various diseases is evident, a problem also declared in Stomatology.
This shortage is evident in this branch of the Medical Sciences; the lack of antibiotics and other medications causes patients pain and stress, in addition to the worries inherent to the disease. That is why the author decided to carry out this research, since it is necessary to promote the use of Natural and Traditional Medicine in health, using the resources that nature provides today in different variants to contribute to the economic health of the country and patients.
For all of the above, the author stated the following scientific problem: How effective will chamomile-argan oil be in the treatment of localized fibro edematous chronic gingivitis in patients between 15 and 19 years old belonging to the Martha Machado Cuní Teacher Training Educational Center on the Isle of Youth?
The results of this research were provided: a study on the effectiveness of chamomile-argan oil in the treatment of localized fibroedematous chronic gingivitis.
This study will encourage stomatologists and the general population to use Natural and Traditional Medicine in treating chronic gingivitis. The aspiration to offer well-being and to increase and preserve the quality of life in the current context from the economic point of view of the population obliges the pertinent use of NTM in the field of Medical Sciences, and especially in the branch of Stomatology, due to the high price of supplies in the international market.
Objective general
To evaluate the effectiveness of Chamomile-Argan Oil in the treatment of Chronic Fibroedematous Gingivitis in patients between 15-19 years old belonging to the "Martha Machado Cuní" Teacher Training Educational Center on the Isle of Youth.
METHOD
An intervention study was carried out with an experimental design, with a pre-test, post-test, and a control group, in patients aged 15-19 belonging to the Teacher Training School "Martha Machado Cuní" of the Special Municipality Isla de la Juventud, between November 2020 and January 2022.
Universe, population, and sample
The study universe consisted of 377 patients between 15 and 19 years of age studying at the Martha Machado Cuní Teacher Training School. The population consisted of 95 patients who presented with gingivitis, and the sample consisted of 68 patients who were identified with localized chronic fibroedematous gingivitis.
The clinical examination carried out at the teaching center selected the patients who participated in the study. Of the total number of patients examined, only those diagnosed with gingivitis were considered to form the population, and the sample consisted of patients diagnosed with localized fibro edematous chronic gingivitis.
The patients who participated in the study were selected using the systematic selection of sample elements to choose the elements that formed the groups of the experiment. This was done based on an interval (K). Thus, of the total number of patients in the sample (N→ 68), the number of patients that made up the groups was (n→ 34), and the interval was (K→ 2). Thus, K=N/n where (N) is the total number of patients, (n) is the sample for each group of the experiment, and (K) is a systematic selection interval. We started randomly using a die according to the number that came out of the roll, which was the initial selection of the list drawn up with the participants in the experiment.
The sample was divided into a control and an experimental group. The experimental groups were randomly assigned to achieve initial equivalence in this experimental design. An unloaded coin was used for the randomization of the groups, and the side of the coin corresponding to each group was designated.
Inclusion criteria of patients in the study
· Be between 15-19 years old and belong to the Escuela Formadora de Maestros "Martha Machado Cuní".
· Present localized fibroedematous chronic gingivitis and agree to participate in the research.
· Do not refer allergies to phytopharmaceuticals.
· To have the authorization of those legally responsible to participate in the investigation.
Research methods
The dialectical materialist method was used to guide the research process, especially the analysis of the dialectical contradiction as the driving source of the development of the object of study, which served as methodological support for the use of other theoretical, empirical and mathematical-statistical methods.
Empirical methods
· Observation: of the stomatognathic apparatus and the school context of the population studied, from which theoretical generalizations were made that facilitated the practice to enrich knowledge and internal elements related to NTM and localized chronic fibroedematous gingivitis were analyzed.
· Documentary analysis: a critical analysis was made of mandatory documents related to NTM, gingivitis and stomatological clinical history.
· Experimental: it made it possible to verify the existing relationships between the elements of the scientific problem and to determine with greater precision the cause-effect relationship between them.
Theoretical methods
They were used for the conceptual interpretation of the empirical data found, to explain the facts, and the essential relationships and fundamental qualities of the phenomenon under study; within these methods were used:
· Analytical-synthetic: it allowed the study of the elements of the problem in their relative independence from each other and also to discover the existing relationships between the elements, as well as the dialectical interaction established between them.
· Inductive-deductive: it made it possible to establish generalizations on the basis of the study of singular phenomena, which made it possible to arrive at certain generalizations that constituted starting points for inferring and confirming theoretical formulations.
· Historical-logical analysis: it allowed to study the trajectory of the facts that have marked important aspects regarding Gingivitis and MNT, in order to show the internal logic of the development of these phenomena, as well as the existing relationship between the use of MNT in the treatment of chronic Gingivitis; taking into account its progressive march towards a deeper, more complete and developed point.
· System approach: it provided the general orientation to study the integral reality in the Isle of Youth and the forms of interaction among the elements that made up the scientific problem.
Mathematical-statistical methods
Descriptive and inferential statistics were used, which allowed the processing of the information gathered through the sources of information, facilitating the generalizations and interpretations to be made from the data. The elaboration and presentation of the results was in tables and figures, which were expressed in absolute and relative frequencies and percentages.
Homogeneity tests were applied using the nonparametric Chi-square analysis statistic to evaluate the relationship between two categorical variables. It was calculated through two-dimensional cross-tabulation tables where each dimension contained a variable with its corresponding categories, with a confidence level of 0 and a degree of freedom of 1.
Selection of variables
Variables: presence of localized fibroedematous chronic gingivitis, sex, age groups, risk factors associated with the appearance of localized fibroedematous chronic gingivitis, effectiveness of chamomile-argan oil.
· Dependent variables: presence of localized fibroedematous chronic gingivitis and effectiveness of treatment.
· Independent variable: chamomile-argan oil and chamomile mouthwash.
· Extraneous variables: age groups.
· Intervening factors: factors associated with the presence of localized fibroedematous chronic gingivitis and sex.
|
Table 1. Operationalization of the variables |
|||
|
Variable |
Type |
Scale |
Description |
|
Presence of chronic fibroedematous gingivitis |
Qualitative Nominal Dichotomous |
Yes No |
According to clinical examination |
|
Sex |
Qualitative Nominal Dichotomous |
Female Male |
According to biological gender to which they belong |
|
Age groups |
Quantitative Continua Simple |
15-16 years 17-19 years old |
According to age at the time of the investigation |
|
Risk factors associated with the presence of localized fibroedematous chronic gingivitis. |
Qualitative Nominal Polytomics |
Smoking Ingestion of foods rich in sugar Hormonal changes Poor oral hygiene |
According to stomatological medical history |
|
Effectiveness of treatment with Natural and Traditional Medicine (chamomile-argan oil and chamomile mouthwashes). |
Qualitative Ordinal Dichotomous |
Satisfactory Unsatisfactory |
According to clinical examination |
Techniques and procedures
An analysis of documents on the topic under study, in both national and international texts, in digital and hard format, was carried out to delimit the problem and substantiate the research topic.
The source used to obtain the information was the stomatological medical record.
With the prior informed consent of the patients who made up the study sample and of those legally responsible and the director of the educational institution, a thorough clinical examination was carried out using a classified set, a millimeter probe, and protective barriers in a stomatological chair on each of the patients who were part of the investigation, to determine the presence of localized chronic fibroedematous gingivitis, during the preparation of the stomatological clinical history. For this purpose, what the patient reported and what was found in the clinical examination using observation, palpation, and probing were taken into account based on the clinical characteristics of the disease described below:
1. Color changes.
2. Changes in size.
3. Changes in shape.
4. Texture changes.
5. Changes in consistency.
6. Contour changes.
7. Changes in position.
8. Presence of gingival hemorrhage.
For the development of the research, chronic gingivitis was classified according to the classification of periodontal disease stipulated in Cuba:
According to the groups of teeth affected:
· Localized: when it affects a single tooth or group of teeth.
· Generalized: when it covers a whole jaw or the whole mouth.
Depending on the different areas of the gum that are affected:
· Marginal gingivitis
· Papillary gingivitis
· Diffuse gingivitis
According to the clinical characteristics of the gingiva:
Edematous gingivitis (ECG)
The gingiva is smooth, shiny, it acquires a bluish-red color and its consistency is soft, the interdental sulcus and marginal sulcus are erased. The beveled shape of the gingiva becomes rounded. If the inflammatory process reaches the attached gingiva there is loss of gingival stippling. Bleeding occurs at the slightest stimulus.
In ECG, virtual pockets may appear at the expense of gingival enlargement without affecting the tissues of the attachment periodontium. Generally this process is painless unless an acute process is added to it. The same occurs in fibroedematous and fibrous gingivitis.
Fibrous gingivitis (FG)
The gingiva is firm, normal color or slightly lighter and hard consistency. There is loss of normal beveling with increased gingival volume. There is no loss of stippling, occasionally there may be reinforcement of the stippling. Bleeding is less marked than in edematous gingivitis.
Fibroedematous gingivitis (FGE)
It presents a combination of the clinical features of edematous and fibrous gingivitis. Clinically, clinical changes of edematous and fibrous gingivitis can be found giving rise to fibro edematous gingivitis. The gingiva may be soft, not hypercolored or red, and firm in consistency.
After the clinical examination of the universe, it was possible to determine the population, consisting of all the patients with gingivitis, and the sample comprised of the patients with localized fibro edematous chronic gingivitis. The author took into account that the sample was only patients with this pathology because it was more feasible to compare the evolution of the disease with the healthy tissue of adjacent regions, in addition to the amount of chamomile-argan oil available. The research groups were treated over 15 days. The experimental group was treated with chamomile-argan oil 3 times a week (single sessions), i.e., six applications during the whole treatment. At the same time, the control group was given fresh chamomile mouthwashes 3 times a day for 15 days.
Weekly consultations were scheduled for evaluation and evolution. For this purpose, the following were considered:
Satisfactory: This group included patients who presented positive signs of the evolution of the disease throughout the investigation, taking into account the properties of phytopharmaceuticals. At the end of the treatment, there were no pathognomonic signs or symptoms of gingivitis.
Unsatisfactory: This group included patients who presented negative signs of the disease's evolution throughout the investigation and unfavorable reactions to the medication used in the study. At the end of the treatment, there were pathognomonic signs or symptoms of gingivitis.
Chamomile and argan essential oil were approved in 2003 by the Working Group on Medicinal Plants, convened by the Pan American Health Organization (PAHO) and the Regional Office of the World Health Organization (WHO), with corresponding registration for use in humans. In the Americas region, the following associations are constituent members of the Working Group:
· MERCOSUR: office in Paraguay.
· ANDEAN COMMUNITY: office in Colombia.
· SICA: office in Guatemala.
· CARICOM: office in Jamaica.
· NAFTA: Canada office.
· ALIFAR: office in Peru.
Oral hygiene was measured quantitatively with the Love Index for dentate patients, which is efficient (less than 20) and deficient (20 or more). To determine this, the patients were asked to practice oral hygiene; then a few drops of Placdent gel were applied to the tongue, instructing them to remove it from the surfaces of the teeth without swallowing it and then to throw it into the spittoon of the dental chair; once the instructions were completed, the efficiency of oral hygiene was calculated using the following equation.
Love Index = Noof dyed surfaces x 100
Surfaces examined
Techniques for processing and analysis of results
The information was collected through the stomatological clinical history. All the information collected was processed digitally, using a computer with Windows 10 as the operating system and Word and Excel programs, both Microsoft Office 2016 applications for the preparation of the text and statistical tables. To evaluate the relationship between two categorical variables, the nonparametric Chi-square analysis statistic was used, taking into account a confidence value of 0 and a degree of freedom of 1. It was calculated using the following equation:
![]()
x²= Chi-square
Oi= observed value
Ei= expected value
Ethical aspects
The data were used confidentially, showing respect for the principle of autonomy of the international code of bioethics for intervention on human beings, were not used for personal purposes, nor were details of this research published that would compromise the integrity of researchers, patients or entities. The information obtained was used by the author for research purposes. The results were presented collectively and not individually. Informed consent was given to the school administration, to those legally responsible and to the patients who participated in the research.
The designed informed consent also provided information on the purposes of the study and appreciation for the cooperation of the participants. The impossibility of to reveal the identity was guaranteed, since it will not present personal identification data. All the information obtained in the research was used only for scientific purposes, in aggregate form and without making allusions to individuals or families so as not to harm the principles of confidentiality.
RESULTS
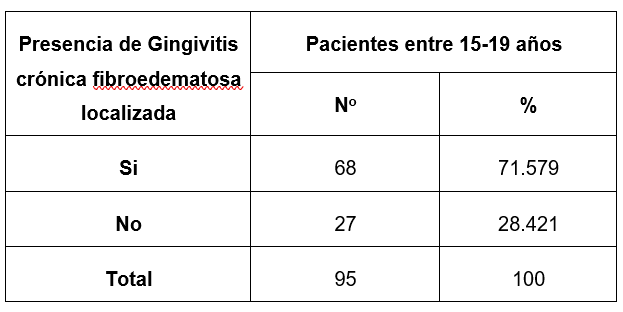
Source: Individual medical history
Figure 1. Distribution according to the presence of localized chronic fibroedematous gingivitis of the population under study belonging to the "Martha Machado Cuní" school, Nueva Gerona. Isla de la Juventud. 2020-2022
Figure 1 shows the distribution of patients according to the presence of localized chronic fibroedematous gingivitis in the study population. As can be seen, 68 patients out of 95 with gingivitis were diagnosed with oral pathology, which represented 71,579 % of the total population.
The results observed in this research show that localized fibro edematous chronic gingivitis is a pathology that significantly affects the adolescent population. After the patients who presented this type of gingivitis were identified, the study sample was formed to develop the research with an experimental design.
The results obtained are consistent with the study conducted by a group of authors(35) in the province of Granma on Epidemiological Characteristics of Chronic Gingivitis in patients aged 5-12 years. Yara, 2017, where out of a universe of 187 patients resulted with the pathology 151 for 80,7 %. But they differ from the study conducted by Castro Yero et al.(36) in the province of Sancti Spíritus, Northern Area, on the characterization of chronic gingivitis in the adolescent population in the period from September 2019 to January 2020, where only 1,6 % of the population resulted with localized fibro edematous chronic gingivitis.
The author considers that the results shown are related to the high presence in unison of risk factors associated with the presence of gingivitis under study. The most significant effort should be to reduce the incidence of localized fibroedematous chronic gingivitis, considering the risk factors through promotional activities in their school environment to favorably influence each student's knowledge, attitudes, and behavior in their daily actions.
Despite all the situations present at the time of the study, the main objective of the research was the treatment of these patients since it presupposes a cure for each individual. Since the patients were sick, it was essential to cure them even if health promotion and prevention activities were carried out concerning this and other pathologies that affect the oromaxillofacial complex. It is worth noting that having diagnosed the patients allowed the sample selection and demonstrated the high incidence of this pathology in adolescents on the Isle of Youth.
While disease promotion and prevention are essential, it is also crucial to cure patients who are ill and to rehabilitate them if necessary. The primary purpose of the present study was to implement a treatment to prevent the pathology from evolving to other periodontal diseases that cause permanent loss of the tooth's supporting tissues.
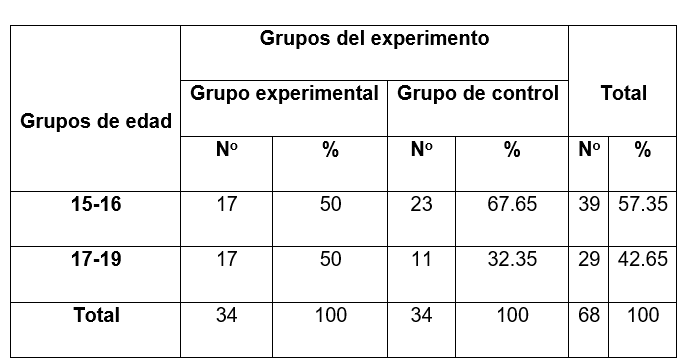
Source: Individual medical history
Figure 2. Distribution according to age of the patients between 15-19 years of age from the "Martha Machado Cuní" school that made up the study sample, Nueva Gerona. Isla de la Juventud. 2020-2022
Figure 2 shows the distribution according to age groups of the experimental groups. As can be seen, the 15-16 age group predominated; of 68 patients, 39 belonged to this age group, for 57,35 % of the total. The scale for the age group variable is the author's work since this scale does not exist in the National Dental Care Program. Adolescents' biological and psychological development was considered in making this division.
The American Academy of Periodontology considers that different periodontal diseases may occur in adolescents as a manifestation of systemic diseases and necrotizing periodontal diseases. Among adolescent gingival diseases, the most prevalent clinical picture is gingivitis associated with antibacterial plaque.(4,5)
Epidemiological, clinical, and histological studies indicate an age-related tendency for gingivitis development. Thus, it has been reported that the severity of gingivitis in children and adolescents with similar amounts of antibacterial plaque3-5 is less extensive than in young adults.
In the literature, figures above 80 % of chronic gingivitis are found in the school population. From second childhood onwards, the number of individuals affected periodontally increases according to Oral Health Surveys carried out in Cuba, as well as epidemiological studies that indicate that the disease increases until puberty.(9,10)
Since the author established the age ranges for the research, there is only coincidence with the study conducted in 2013 by Villegas Rojas et al.(37) at the Clínica Estomatológica Docente 27 de noviembre, in Matanzas, where patients between 15 and 16 years of age represented the highest percentage.
The results differ from the study conducted by Dr. Mayelín Ferrales Escalona* on the Treatment of Chronic Edematous Gingivitis with pendejera root in adolescents. Policlínico Docente Universitario "Juan Manuel Páez Inchausti," 2018, where patients between 15 and 16 years of age were the least represented in the research, with six patients.
In the author's opinion, age is one aspect to be taken into account and of great relevance in the research carried out since it allows, due to the characteristics of the groups, the identification of the different risk factors presented by the group. At the same time, it contributes to directly treating these factors that may or may not modify the research results.
Adolescence is the best time to form beneficial habits based on what the individual recognizes as positive for maintaining the balance of the health-disease process. This is linked to motivation and awareness, which, from the psychological point of view, are essential links for incorporating adequate knowledge, thus achieving positive changes in behavior and healthy lifestyles that increase the quality of life.
Because of the importance of knowing about periodontal diseases and their consequences on health, it is necessary to direct promotion and prevention activities mainly toward age groups with full learning capacity and where one of these pathologies has not yet appeared. To prevent the appearance of periodontal diseases, a high culture of health education is needed in the community, thus avoiding the need to resort to secondary care services, which are more costly for the institution, require more resources, and are increasingly demanded by patients.
In addition, stomatologists must take up the challenge if we want people to reach the so-called "third age" with quality of life. This is ensured as long as adolescents have a high-risk perception of these pathologies and the incidence of these pathologies in the young and adult population gradually decreases.
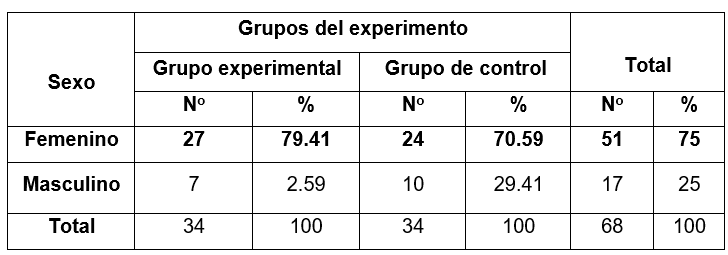
Source: Individual medical history
Figure 3. Distribution according to sex of patients between 15-19 years of age from the "Martha Machado Cuní" school that made up the study sample, Nueva Gerona. Isla de la Juventud. 2020-2022
Figure 3 shows the distribution according to sex of the experimental groups, with a predominance of the female sex with a total of 51 patients, which represented 75 % of the total sample. In both experiment groups, females predominated, guaranteeing compliance with the initial equivalence and the internal validity necessary for any experiment.
Some authors have pointed out that sex influences the variations that the periodontium may experience. They state that when evaluating the influence of female hormones on the clinical manifestations of periodontal diseases, estrogen and progesterone levels modulate the host's inflammatory response to bacterial aggressions.(4,5) Female hormones alone are insufficient to produce gingival alterations; however, they can alter the response of periodontal tissues to antibacterial plaque and contribute directly to periodontal disease.
The results of the present investigation coincide with those obtained by Dr. Yousemy Álvarez Romero** in her study on the Behavior of periodontal disease in a dental office. Venezuela, 2006, where female sex predominated, with 57,1 % representing 116 patients. They also coincide with the studies carried out by Dr. Yaradí Rizo Fernández*** in 2017 in the Special Municipality Isla de la Juventud titled Periodontal situation of older adults belonging to office 23 of the Stomatological Clinic 41, where out of a sample of 120 patients 86 were female for 71,7 % of the total.
There is a coincidence with the results of the study conducted by Dr. Mayelín Ferrales Escalona* on the Treatment of Chronic Edematous Gingivitis with pendejera root in adolescents. Policlínico Docente Universitario "Juan Manuel Páez Inchausti," 2018, where the female sex was predominantly represented by 18 patients for 60 % of the sample. It also coincides with a study conducted in 2017-2019 by Dr. Katia Rivero Guerra39 at the "3 de Octubre" Provincial Stomatological Clinic in the Tunas municipality on laser therapy in edematous chronic gingivitis where the female sex predominated.
The studies conducted by Castro Yero et al.(36) in the province of Sancti Spíritus, Northern Area, on the characterization of chronic gingivitis in the adolescent population in the period from September 2019 to January 2020 and Hilda Lídice Zaldívar Bernal et al.(39) on Behavior of chronic gingivitis in adolescents of the "Jesús Fernández" Basic Secondary School, in Santa Marta, Cárdenas, do not coincide with the results of the present research where the male sex was predominant.
More women than men have been born on the Isle of Youth for several decades, so this sex predominates in the study sample. The development of this research is significant because women have a greater perception of risk concerning health care and practice a hygienic-sanitary culture in their daily lives. Men are more exposed to multiple risk factors that threaten the patient's general health due to their daily lifestyle, causing a gradual deterioration in health.
The author considers that the predominance of the female sex is beneficial since it plays a fundamental role in differential exposure to risk. They also have an essential share in the weight they have to face risks, protect their health, and influence the direction of the health development process. It is necessary to highlight the role played by women in the proper maintenance of health, both general and oral, because it is precisely she who is responsible for creating in the nucleus where she is, behaviors, habits, and customs that favor health, which will be followed by the members of the group and integrated into their system of knowledge about what to do to maintain health.
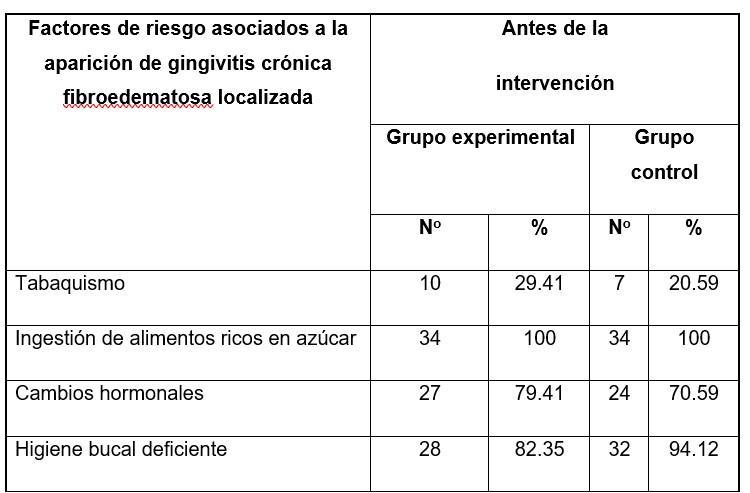
Source: Individual medical history
Figure 4. Distribution according to risk factors associated with the appearance of localized fibroedematous chronic gingivitis before the intervention in the study sample, Nueva Gerona. Isla de la Juventud. 2020-2022
Figure 4 shows the distribution according to risk factors associated with the appearance of localized fibro edematous chronic gingivitis in the experimental groups before the intervention. As can be seen in the present study, the risk factor that predominated in the two groups of the experiment before the intervention was ingesting foods rich in sugar, with 100 % in the two groups. The consumption of this type of food, depending on the frequency with which it is ingested and the hygienic habits of the patients, favors the formation of antibacterial plaque. Antibacterial plaque has been directly related throughout history with diseases affecting the periodontium; for many authors, the microorganisms present in this entity are the main causal agents of gingivitis.(3)
Poor oral hygiene was the second risk factor, with the highest incidence in the investigation in both groups, represented by a considerable percentage. Neglecting oral hygiene leads to bacterial growth that can lead to the appearance of dental caries and periodontal diseases.
Hormonal changes are latent risk factors in adolescence. At puberty, these changes predispose these patients to periodontal conditions such as gingivitis. Increased estrogen and progesterone levels can increase gingival irrigation and modify the response of gingival tissue to oral biofilm, favoring gingival inflammation and gingival bleeding during toothbrushing.(9)
Smoking has been defined as the leading preventable cause of mortality, causing more deaths than Acquired Immune Deficiency Syndrome, alcoholism, and traffic accidents. Smoking is indeed a significant risk factor for the development of periodontal diseases. Patients who smoke are more prone to suffer from this type of disease than non-smokers.(9,10)
The results of the present investigation differ from those of the study conducted by a group of authors(35) in the province of Granma on Epidemiological Characteristics of Chronic Gingivitis in patients aged 5-12 years. Yara, 2017, where poor oral hygiene predominated as a risk factor, representing 58,7 % of the total sample studied. They also differ from the study conducted by Vázquez et al.(40) on risk factors associated with the occurrence of periodontal disease from January to December 2019 at the David Moreno Domínguez Polyclinic in Santa Rita, Jiguaní, Granma.
There are discrepancies between the studies conducted by Castro Yero et al.(36) in the province of Sancti Spíritus, Northern Area, on the characterization of chronic gingivitis in the adolescent population in the period from September 2019 to January 2020 and Zaldívar Bernal et al.(39) on Behavior of chronic gingivitis in adolescents of the "Jesús Fernández" Basic Secondary School, in Santa Marta, Cárdenas, where the intake of foods rich in sugar was not the predominant risk factor.
It also differs from the study conducted by Dr. Mayelín Ferrales Escalona* on the Treatment of Chronic Edematous Gingivitis with pendejera root in adolescents, Policlínico Docente Universitario "Juan Manuel Páez Inchausti," 2018, where poor oral hygiene was the predominant risk factor in 100 % of the population under study.
Different risk factors lead to periodontal disease, specifically localized chronic fibro edematous gingivitis. The factors described above were those determined at the beginning of the investigation.
The author considers that stomatologists' most important work should be aimed at modifying harmful lifestyles in the population through educational interventions. In addition, the author agrees with the criterion supported by research that states that controlling risk factors is necessary for the prevention of periodontal diseases.
In this sense, health promotion plays a crucial role in counteracting the non-specific phase of the disease, i.e., to prevent the possible incidence of the risk factors that favor the appearance of these pathologies. The accumulation of risk factors in the same patient thus constitutes a risk factor of greater power and predictive capacity than any risk factors considered individually.
If this cumulative effect is carried out by weighting the predictive power of each factor, this trend is maintained, and the sensitivity and specificity of the multifactorial risk index increase. The presence of a conglomerate of risk factors associated with the appearance of periodontal diseases is the cause of a high level of risk of suffering these pathologies.
Identifying them is useful for carrying out effective health promotion activities. Thus, identifying each risk factor would organize primary preventive measures and highlight those that require specific protection both in the patient and in his or her school and family environment.
Stomatologists currently face the challenge of identifying patients at risk of disease and detecting the disease early. This allows for measuring each individual's probability of developing periodontal disease.
This knowledge for stomatologists constitutes a guide for educational and preventive work with patients in the community. Although the primary purpose of the present research was to implement a drug therapy using chamomile-argan oil, educational talks were always given during disease promotion and prevention activities to avoid the appearance of other pathologies or a future recurrence of the disease under study.
Although the research had a therapeutic rather than preventive orientation, the author considers it a reservoir of information for future studies on localized fibroedematous chronic gingivitis. She also believes that the present research is only a beginning in the therapeutic use of chamomile-argan oil. The data on risk factors associated with localized fibro edematous chronic gingivitis in the Martha Machado Cuní Teacher Training School adolescents are collected for later use in future studies on this pathology.
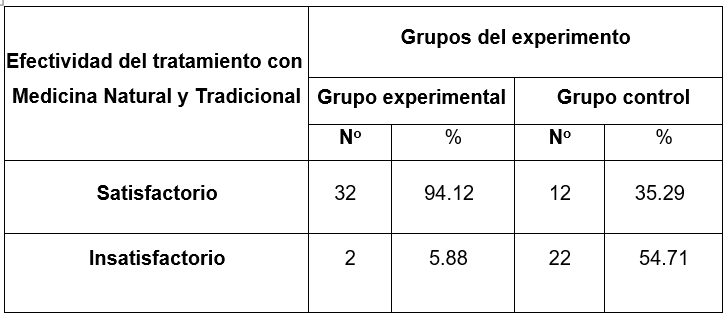
Source: Individual medical history. X2 =44 Gl=1 p=0
Figure 5. Distribution according to effectiveness of treatment with Natural and Traditional Medicine of patients between 15-19 years of age from the "Martha Machado Cuní" school who made up the study sample, Nueva Gerona. Isla de la Juventud. 2020-2022
Figure 5 shows the effectiveness of treatment with MNT of the patients who made up the study sample. It is important to note that both groups of the experiment were treated with MNT; the experimental group was treated with chamomile-argan oil, and the control group was treated with chamomile mouthwash. The principles of medical ethics were considered, and both groups were treated, even if the aim was only to evaluate the effectiveness of chamomile-argan oil. Dividing the sample into two groups made it possible to statistically demonstrate the efficacy of the chamomile-argan oil treatment while still establishing therapy for the patients in the control group.
As previously explained, the treatment with chamomile-argan oil was applied as a therapy in the experimental group, and the table shows that out of a total of 34 patients who made up this group, 94,12 % of them obtained satisfactory results in the total cure of the pathology in question. The control group indicated fresh chamomile mouthwashes, and it can be observed that in that group, only 12 patients were satisfactorily cured, representing 39,29 % of the total group of 34 patients. After applying the statistics, it was possible to demonstrate that chamomile-argan oil effectively treated localized chronic fibro edematous gingivitis since the variables were significantly related.
The author considers it relevant that the treatment was carried out in two weeks in both groups of the experiment. Six sessions of single applications were carried out in the experimental group, while the control group was treated with three daily applications in the same period.
It is important to emphasize that the applications of the first group were provided by the researcher, while the second group had to self-administer their doses. Thus, the treatment of the latter was subject to each patient's availability of time and linked to the responsibility of each of them and their legal guardians.
The progress and considerable scientific development that Stomatology has undergone in this century is the product of numerous factors that have systematically sought the application of basic sciences to the development of clinical work, transforming clinical technicality into a science of knowledge, preservation, and recovery of the health of the stomatognathic apparatus. In the study, the favorable results of using chamomile-argan oil were evident since the properties of the medicine against the pathology studied are convincing, propitiated by a natural synergism, potentiating the effect of the components of the natural medicine used in the research.
There are a few published studies on treating localized fibro edematous chronic gingivitis pathology with chamomile-argan oil, so comparing the results obtained is scarce. The present study's results agree with those of the one carried out by Cosco Robles(41) in Lima, Peru, on the inhibitory action of chamomile oil in pediatric patients, where 52 % of the population showed satisfactory results.
The differences observed according to the treatment used allowed us to endorse the significance of the results obtained in the research in a short period, which is why the author considers that the intervention has a high impact and infinite usefulness in terms of the economy and health. In addition to providing a more effective therapy, it complies with the guidelines established in the policy of the Cuban State and indicators of the Ministry of Public Health of the Republic of Cuba.
CONCLUSIONS
· Localized fibroedematous chronic gingivitis predominated in the study population.
· Female patients and those aged 15-16 years predominated in the study sample.
· Sugar-rich food intake, poor oral hygiene and hormonal changes were predominant factors associated with the development of localized fibroedematous chronic gingivitis.
· Chamomile-argan oil is effective in the treatment of localized fibroedematous chronic gingivitis.
RECOMMENDATIONS
It is recommended to make use of the different modalities of Natural and Traditional Medicine, especially in our Special Municipality Isla de la Juventud, in order to contribute to the economy of the country that today is going through a difficult situation. It is necessary to exploit the green world that surrounds us as long as the therapeutic purposes are covered.
BIBLIOGRAPHIC REFERENCES
1. Compendio de Periodoncia. La Habana: Ciencias Médicas; 2006.
2. Pérez OR, Sánchez Huerta HA, Corona Zavala A. Prevalencia y severidad de enfermedad periodontal crónica en adolescentes y adultos. Oral. 2011;12(39):799-804. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75072011000300009&lng=es
3. Araújo MG. Epidemiología de la enfermedad periodontal en América Latina. Rev Fundac Juan Jose Carraro. 2010;15(31):32-36.
4. Zaror Sánchez C, Muñoz Millán P, Sanhueza Campos A. Prevalencia de gingivitis y factores asociados en niños chilenos. Av Odontoestomatol. 2012;28(1). http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-12852012000100005&lng=en&nrm=iso&tlng=en
5. Lagos Lagos A, Juárez Membreño IA, Iglesias Gómez M. Necesidad de tratamiento periodontal e higiene oral en adolescentes de 12 años de Llanquihue. Rev Clin Periodoncia Implantol Rehabil Oral. 2014;7(2). http://www.scielo.cl/scielo.php?script=sci_arttext&pid=S0719-01072014000200005
6. Matesanz-Pérez P, Matos-Cruz R, Bascones-Martínez A. Enfermedades gingivales: una revisión de la literatura. Av Periodoncia. 2008;20(1). http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1699-65852008000100002
7. Cuba. Ministerio de Salud Pública. Dirección Nacional de Estomatología. Estado de salud bucal. Evaluación de la situación en Cuba. La Habana: Ciencias Médicas; 2007.
8. Pérez Hernández LY, De Armas Cándano A, Fuentes Ayala E, Rosell Puentes F, Urrutia Díaz D. Prevalencia de enfermedad periodontal y factores de riesgo asociados. Policlínico "Pedro Borrás", Pinar del Río. Rev Cienc Méd Pinar Río. 2011;15(2). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-31942011000200006&lng=es&nrm=iso&tlng=es
9. Doncel Pérez C, Vidal Lima M, Del Valle Portilla MC. Relación entre la higiene bucal y la gingivitis en jóvenes. Rev Cub Med Mil. 2011;40(1):40-47. http://scielo.sld.cu/pdf/mil/v40n1/mil06111.pdf
10. Pérez Barrero BR, Sánchez Zapata R, Gondín Gener M, Sánchez Garrido AV. Estado periodontal de pacientes jóvenes atendidos en la Clínica Estomatológica Vista Alegre. Medisan. 2012;16(4). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192012000400007&lng=es&nrm=iso&tlng=es
11. Cardentey García J, Silva Contreras AM, Pulido Valladares Y, Arencibia García E, Martínez Cabrera M. Caracterización de la salud bucal en la adolescencia en un área de salud. Rev Cienc Méd Pinar Río. 2011;15(3). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-31942011000300003&lng=es&nrm=iso&tlng=es
12. Carranza FA, Newman MG. Periodontología clínica. 9na ed. México: McGrawHill Interamericana; 2002.
13. Iglesias Berlanga GE, Iglesias Berlanga IJ, Pérez Báez N, González Iglesias A. Estado periodontal en adultos jóvenes del área Cangre del municipio de Güines. Rev Cienc Méd Habana. 2012;18(1). http://revcmhabana.sld.cu/index.php/rcmh/article/view/558/html
14. Pérez Barrero BR, Duharte Garbey C, Perdomo Estrada C, Ferrer Mustelier A, Gan Caldero B. Higiene bucal deficiente, hábito de fumar y gingivitis crónica en adolescente venezolanos de 15-18 años. Medisan. 2011;15(9):1189. http://scielo.sld.cu/pdf/san/v15n9/san01911.pdf
15. Bellón Leyva S, Aldama Bellón Y, Echarry Cano O. Aplicación de la Medicina Natural y Tradicional en Estomatología. En: González Naya G, Montero del Castillo ME, editores. Estomatología General Integral. La Habana: Editorial Ciencias Médicas; 2013. p. 377-89.
16. Hernández Falcón Larisa, García Rodríguez Ileana, Garay Crespo María I. Manual de terapias naturales en estomatología. La Habana: Ed Ciencias Médicas; 2011.
17. Gispert Abreu Estela, Cantillo Estrada Elena, Rivero López Aracelys, Oramas Rodríguez Berta. Crema dental con manzanilla, efecto estomatológico. Rev Cubana Estomatol. 1998;35(3):107-111. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75071998000300007&lng=es
18. García Bacallao Lourdes, Rojo Domínguez Delia Mercedes, García Gómez Luis Vicente, Hernández Ángel Maureen. Plantas con propiedades antiinflamatorias. Rev Cubana Invest Bioméd. 2002;21(3):214-216. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-03002002000300012&lng=es
19. Morón Rodríguez Francisco, Furones Mourelle Juan, Pinedo Gutiérrez Zulima. Actividad espasmolítica del extracto fluido de Matricaria recutita (manzanilla) en órganos aislados. Rev Cubana Plant Med. 1996;1(1). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-47961996000100005&lng=es
20. Vara-Delgado Ana, Sosa-González Rodolfo, Alayón-Recio Clara Sonia, Ayala-Sotolongo Nismely, Moreno-Capote Giselle, Alayón-Recio Virginia del Carmen. Uso de la manzanilla en el tratamiento de las enfermedades periodontales. AMC. 2019;23(3):403-414. http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1025-02552019000300403&lng=es
21. García Milián AJ, Morón Rodríguez F, Alonso Carbonell L, López Puig P, Ruiz Salvador AK. Estrategia para lograr un uso racional de los medicamentos herbarios. Rev Cubana Plant Med. 2005;10(2). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-47962005000200014&lng=es
22. Álvarez Díaz AT, Tosar Pérez MA, Echemendía Sálix C. Medicina Natural y Tradicional. Acupuntura, moxibustión y medicina herbolaria. La Habana: Editorial Ciencias Médicas; 2017.
23. Krapp K, Longe J. Enciclopedia de Medicinas Alternativas. España: Editorial Océano; 2000. Fitoterapéuticos; p. 605.
24. Frías Tamayo JA, Ramírez Peña G, Paz Lorente C de la, Herrero Pacheco C, Acosta Campusano Y. Sechium edule (jacq) sw: Efecto Inmediato de Infusiones de Consumo Habitual en las Propiedades Salivales. Medisur. 2016;14(6). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1727-897X2016000600002&lng=es
25. Rodríguez Moreno AM, Arcia Cruz L, Moreno Diéguez O, Andrés Medina A, Rojas Pérez LM. Eficacia y seguridad de la tintura de manzanilla en el tratamiento de la gingivitis crónica edematosa. Multimed. 2016;20(5). http://www.medigraphic.com/pdfs/multimed/mul-2016/mul165h.pdf
26. Villate Gómez F. Consideraciones de la medicina tradicional en su combinación con la medicina occidental y el enfoque diagnóstico. Rev Cub Med Mil. 2013;42(1). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0138-65572013000100016&lng=es
27. Cardentey J. Empleo de la medicina natural y tradicional en el tratamiento estomatológico. Arch Med Camagüey. 2015;19(3). http://www.scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-34662013000300010&lng=es
28. Villar López L, Mesa Ramos M, Pimentel OG. Manual de Fitoterapia. Lima: Organización Panamericana de Salud; 2001. http://www.bvsde.paho.org/texcom/manualesMEC/fitoterapia/fitoterapia.html
29. Morón Rodríguez F. Las plantas medicinales, la medicina y los sistemas de salud. Rev Cubana Plant Med. 2012;17(3). http://www.scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-47962012000300001
30. Martínez Ávila Y, Gómez López LL. Impacto social de una estrategia de intervención sobre prescripción racional de medicina verde en Céspedes durante 2011. Rev Cubana Plant Med. 2013;18(4). http://www.scielo.sld.cu/scielo.php?pid=S1028-47962013000400012&script=sci_arttext&tlng=en
31. García Salman JD. Consideraciones sobre la Medicina Natural y Tradicional, el método científico y el sistema de salud cubano. Rev Cubana Salud Pública. 2013;39(3). http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-34662013000300010&lng=es
32. Martínez SM, Andrade DJ. Guía de Árboles Nativos de la provincia de Salta. Ed. Ministerio de Educación de la provincia de Salta; 2006. 187 p.
33. Marzocca A. Nociones Básicas de Taxonomía Vegetal. Ed. IICA. San José. Costa Rica; 1985. 263 p.
34. Rueda Robles A. Estudio de la composición y de las propiedades antioxidantes del aceite de argán virgen extra. España; 2015.
35. Colectivo de Autores. Características Epidemiológicas de la Gingivitis Crónica en pacientes entre 5-12 años. Granma, Yara; 2017. https://search.scielo.org/?lang=pt&q&au:Gil-González,%20Diana
36. Castro Yero JL et al. Caracterización de la gingivitis crónica en la población adolescente en el período comprendido entre septiembre de 2019 a enero de 2020. Sancti Spíritus, Área Norte; 2019. https://revgaleno.sld.cu/index.php/ump/article/view/606
37. Villegas Rojas IM, Herrada Soto Y, Reyes Martín B. Factores de riesgos de la gingivitis crónica en estudiantes de 15 a 18 años. Clínica Estomatológica Docente 27 de noviembre, Colón, Matanzas; 2013. https://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242016000300004
38. Rivero Guerra K. Laserterapia en la gingivitis crónica edematosa 2017-2019. Clínica Estomatológica Provincial “3 de Octubre”. Municipio Las Tunas; 2017. https://www.eumed.net/rev/caribe/2019/12/laserterapia-gingivitis-cronica.html
39. Zaldívar Bernal HL. Comportamiento de la gingivitis crónica en adolescentes de la Secundaria Básica Jesús Fernández. Santa Marta, Cárdenas, Matanzas; 2014. https://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18242014000700004
40. Fonseca Vázquez M, et al. Factores de riesgos asociados a la aparición de la enfermedad periodontal de enero a diciembre de 2019 en el Policlínico David Moreno Domínguez de Santa Rita. Granma, Jiguaní; 2019. https://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1028-48182021000300013
41. Cosco Robles DA. Acción inhibitoria del aceite de manzanilla en pacientes pediátricos. Facultad de Odontología de la Universidad de San Marcos, Lima, Perú; 2010. https://pesquisa.bvsalud.org
FINANCING
None.
CONFLICT OF INTEREST
None.
AUTHORSHIP CONTRIBUTION
Conceptualization: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Data curation: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Formal analysis: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Research: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Methodology: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Project management: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Resources: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Software: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Supervision: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Validation: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Display: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Drafting - original draft: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.
Writing - proofreading and editing: Rosa María Montano-Silva, Yoneisy Abraham-Millán, Aliana Peña-Méndez, Yousemy Álvarez-Romero, Darianna Rubio-Díaz, Aliannys González-Alvarez.