doi: 10.56294/nds202240
ORIGINAL
Nursing care related to
quality of life in diabetic patients treated at a hospital in North Lima
Cuidados de enfermería
sobre la calidad de vida en pacientes diabéticos atendidos en un hospital de
Lima Norte
David Hugo Bernedo-Moreira1  , Alfredo Giovanni Lazo-Barreda2
, Alfredo Giovanni Lazo-Barreda2  , Paul Espiritu-Martinez3 , César Carbache Mora4
, Paul Espiritu-Martinez3 , César Carbache Mora4  *,
Aaron Samuel Bracho Mosquera5 *
*,
Aaron Samuel Bracho Mosquera5 *
1Universidad
César Vallejo. Lima, Perú.
2Universidad
Nacional de San Agustín de Arequipa. Perú.
3Universidad
Nacional Autónoma Altoandina de Tarma. Junín, Perú.
4Universidad
Laica Eloy Alfaro de Manabí. Ecuador.
5Universidad
de Panamá. Panamá.
Cite as:
Bernedo-Moreira DH, Lazo-Barreda AG, Espiritu-Martinez P, Carbache Mora C,
Bracho Mosquera AS. Nursing care related to quality of life
in diabetic patients treated at a hospital in North Lima. Nursing Depths
Series. 2022; 1:40. https://doi.org/10.56294/nds202240
Submitted:
14-02-2022 Revised: 05-05-2022
Accepted: 23-07-2022 Published: 24-07-2022
Editor: Dra.
Mileydis Cruz Quevedo
Corresponding Author: César Carbache Mora *
ABSTRACT
Diabetes mellitus is one of the leading
diseases worldwide that significantly compromises a person’s health and
diminishes their quality of life over time. Therefore, the objective of this
research is to determine the nursing care provided to diabetic patients treated
at a hospital in northern Lima and its impact on their quality of life. This is
a quantitative, descriptive, cross-sectional study with a total population of
132 patients who completed a sociodemographic data questionnaire and the
Diabetes 39 instrument. The results show that 58,8 % of patients aged 30 to 59
have an average quality of life. In conclusion, educational counseling on
personal care should be provided to patients with diabetes mellitus.
Keywords: Quality of Life; Diabetes Mellitus; Nursing Care; Noncommunicable
Diseases.
RESUMEN
La diabetes mellitus a
nivel mundial es una de las enfermedades principales en las que compromete
considerablemente el estado de salud de la persona y disminuye con el tiempo su
calidad de vida, por lo que el objetivo de investigación es determinar los
cuidados de enfermería sobre la calidad de vida en pacientes diabéticos
atendidos en un hospital de Lima Norte. Es un estudio cuantitativo,
descriptivo-transversal, con una población total de 132 pacientes que
desarrollaron un cuestionario de datos sociodemográficos y el instrumento
Diabetes 39. En sus resultados, observamos que entre las edades de 30 a 59 años
de edad el 58,8 % tienen una calidad de vida media. En conclusión, se debe
realizar consejerías educacionales sobre los cuidados personales en pacientes
con diabetes mellitus.
Palabras clave: Calidad
de Vida; Diabetes Mellitus; Cuidados de Enfermería; Enfermedades no
Transmisibles.
INTRODUCTION
Diabetes mellitus (DM)
is a metabolic disease that affects the population and is considered one of the
major public health problems today.(1) Population aging, increasing
urbanization, sedentary lifestyle, inadequate diet and obesity are largely
responsible for the increasing incidence and prevalence of DM, which represents
a challenge for health services.(2)
Quality of life (QoL)
is considered a good indicator of life expectancy, especially for people with
special health conditions, in addition to improving patient care and disease
management, particularly during the coronavirus pandemic (COVID-19), future
implementation may also improve the quality of life of people with diabetes
mellitus.(3)
Given that knowledge
about the disease and the attitude adopted towards DM self-care have been
linked to QoL,(4) it is believed that the more knowledge an
individual has about the disease and its treatment, the more likely they are to
adopt positive attitudes, which translates into aspects that can be directly or
indirectly reflected in their QoL.(5,6)
Diabetes distress is
known to be a problem related to diabetes care, access to social support and
care, and emotional stress and anxiety. This often includes the concerns,
fears, and threats associated with the demands of a chronic disease such as
diabetes.(7)
In
the United States, a study confirmed that diabetes distress (DD) is associated
with lower diabetes quality of life (QoL) for people with type I and type II
diabetes, suggesting that attending or working in the teaching field may be
associated with high diabetes distress scores and lower diabetes QoL.(8)
A study in Cuba of 82
people with type II diabetes in the city of Teresina revealed that most people
living with diabetes have good QoL, and those who suffer a negative impact have
the emotional factor as the most affected domain. Among the sociodemographic
and clinical conditions associated with low QoL, age, type of housing, type of
diabetes, and time since diagnosis of the disease stood out.(9)
A study in Mexico that
evaluated 27 patients diagnosed with type II DM showed that the highest level
of quality of life is reflected in social and professional care, satisfaction
with treatment, and the impact on treatment, while the most affected aspects
were general well-being and concern about the future effects of diabetes. In
addition, a small, positive, and statistically significant correlation was
found between disease progression time and adverse treatment effects.(10)
In Asia, a study
conducted in Iran, where 266 older people with type II diabetes were surveyed,
revealed that barriers to treatment such as psychological distress related to
diabetes management, type of treatment, and age were statistically significant
predictors of QoL dimensions.(11) On the other hand, a study among
DM patients living in central Thailand in 2019 showed that more than half of DM
patients had a good quality of life.(12)
A study conducted in
Spain showed that women's quality of life in terms of health is worse than that
of men. Age, number of years since diagnosis, presence of complications, as
well as comorbidities, medication regimens, and glycemic control all have a
direct impact. On the other hand, living alone, low socioeconomic status, low
social support, and needing help with diabetes were associated with poor
quality of life.(13)
In Africa, in
southwestern Ethiopia, it was noted that all dimensions of HRQoL in diabetic
patients were affected in this study environment, with important predictors
such as age, disease duration, and fasting glucose levels being identified.
Interventions beyond standard care are needed to improve HRQoL in people with
diabetes.(14)
In
Latin America, a study conducted in Brazil found that DM has a high impact on
patients' QoL, with the main correlated variables being age, sex, time of
diagnosis, glycemic control, and the presence of complications/comorbidities.(15)
Similarly, in Peru, a study found a
significant association between the level of knowledge about DM2 and the level
of adherence to DM2 treatment, as well as the level of education and place of
origin, indicating the importance of determining certain factors specific to a
population that directly influence adherence to treatment for this disease.(16)
Therefore, the research
objective is to determine the nursing care provided to diabetic patients
treated at a hospital in northern Lima.
METHOD
Research type and design
This study is
quantitative in nature, using a descriptive, cross-sectional, non-experimental
methodology.(17)
Population
The population consists
of a total of 132 participants diagnosed with diabetes mellitus who are receiving
care at a hospital in northern Lima.
Inclusion Criteria
·
Participants must be over 30 years of age.
·
Participants who are treated at the endocrinology clinic.
·
Participants who voluntarily agree to participate in the study.
Technique and Instrument
The technique used was
a survey, which describes the data collection instrument Diabetes 39.
For data collection,
the survey is distributed according to sociodemographic aspects and the
Diabetes 39 instrument, which comprises 39 items distributed across five
dimensions: energy and mobility (15 items), diabetes control (12 items),
control and concern (4 items), social burden (5 items), and sexual function (3
items). These were assessed using a Likert scale with seven response options:
"1 = not at all," "2 = almost not at all," "3 = a
little," "4 = fair," "5 = a lot," "6 = too
much," and "7 = tremendously," so that the score would range
from "1 to 91" for low quality of life, "92 to 183" for
average quality of life, and "184 to 273" for high quality of life, with
higher scores indicating a higher quality of life for the patient. Finally, two
items at the end (patient perception and severity of the disease) were not
taken into account as they do not contribute to the final score.(18,19)
The instrument was
validated using the Kaiser-Mayer-Olkin sample adequacy test, obtaining a
coefficient of 0,965 (KMO > 0,5), and the Bartlett sphericity test yielded
significant results (X2approx. = 9497,375; gl = 741; p = 0,000).
The reliability of the
instrument was assessed using Cronbach's alpha, obtaining a score of 0,989 (α
> 0,8) for the 39 items of the instrument.
Place and Application of the Instrument
To conduct the survey,
prior arrangements were made with the head of outpatient endocrinology to carry
out the study, and details were provided so that they would be aware of what
was going to be done.
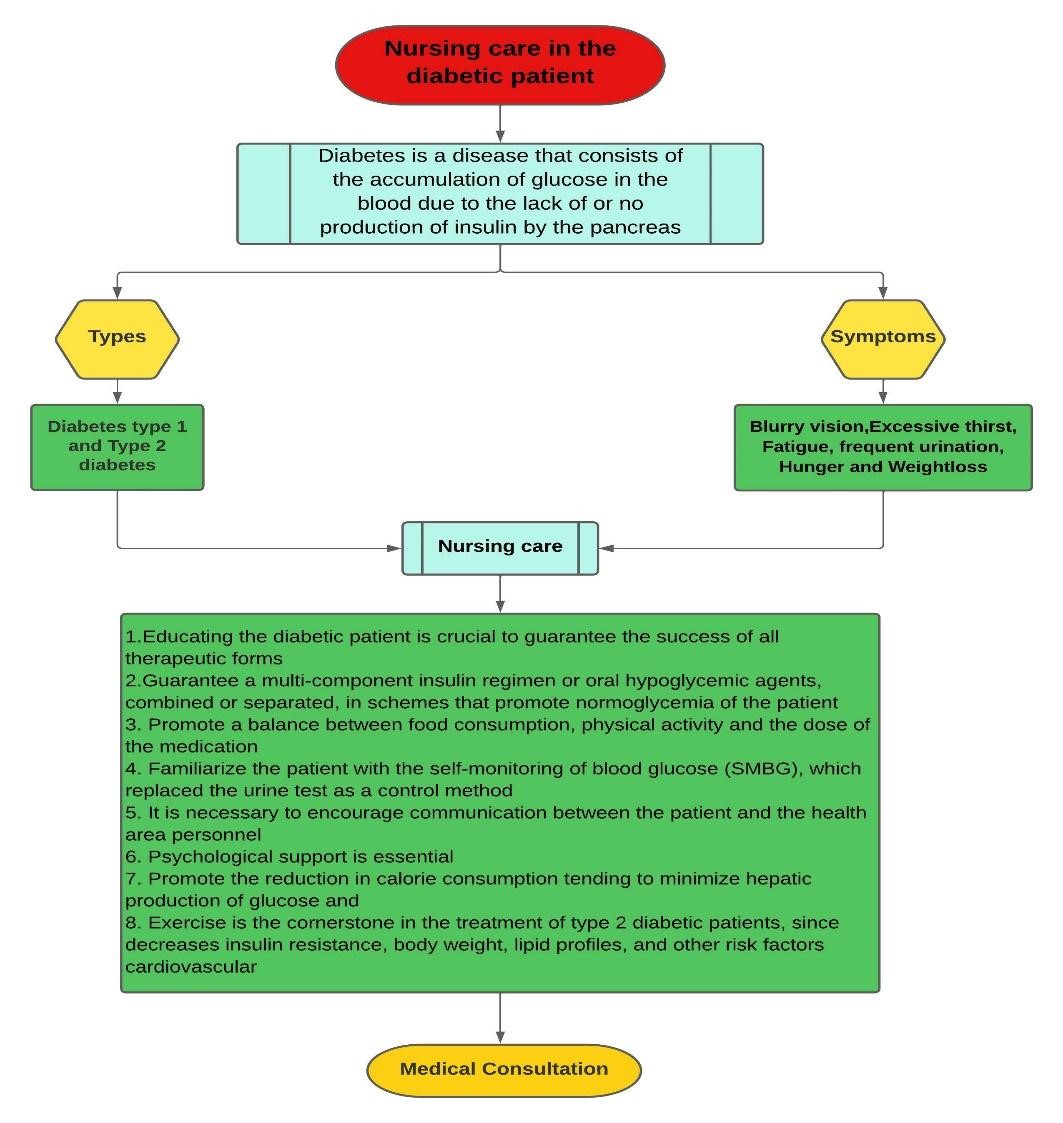
Figure 1.
Flowchart of nursing care for a diabetic patient
This flow chart shows
the process that nursing professionals must follow when caring for patients
diagnosed with diabetes mellitus.
The importance of blood
glucose control in reducing complications in diabetic patients has been clearly
demonstrated in long-term studies and interventions, where the primary goal of
blood glucose control in most diabetics is to reduce glycosylated hemoglobin to
less than two percentage points above the upper limit of normal. In addition,
the intensity of treatment must be individualized and adjusted in each case. In
the care of diabetic patients, it is essential to simultaneously manage other
metabolic variables that coexist with hyperglycemia, i.e., serum cholesterol,
HDL cholesterol, LDL cholesterol, and triglyceride concentrations must be
strictly monitored, as well as weight, body mass index (BMI), waist-to-hip
ratio, and systolic and diastolic blood pressure, in order to minimize the
incidence of acute and chronic complications.
To this end, nursing
care includes assessment and control of symptoms, but also adequately informing
the patient about the medical, nutritional, and physical guidelines to follow
for self-treatment of their disease.
RESULTS
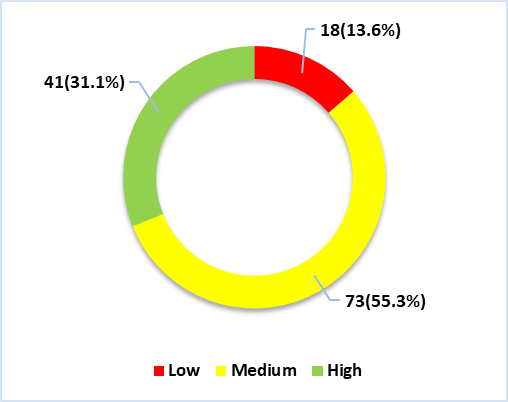
Figure 2. Quality
of life in diabetic patients treated at a hospital in northern Lima
We can see in figure 2
that 13,6 % (n=18) of participants have a low quality of life, 55,3 % (n=73)
have an average quality of life, and 31,1 % (n=41) have a high quality of life.
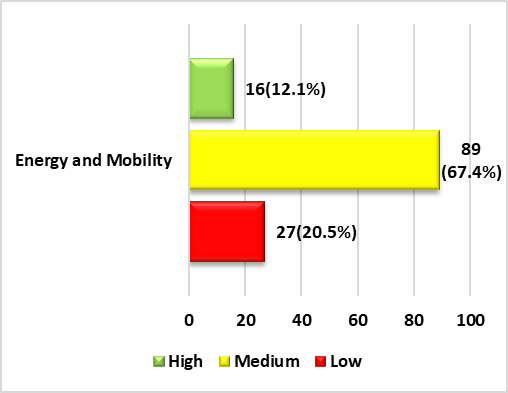
Figure 3. Quality
of life in terms of energy and mobility in diabetic patients treated at a
hospital in northern Lima
In figure 3, we can see
that 12,1 % (n=16) of participants have a high quality of life in terms of
energy and mobility, 67,4 % (n=89) have an average quality of life, and 20,5 %
(n=27) have a low quality of life.
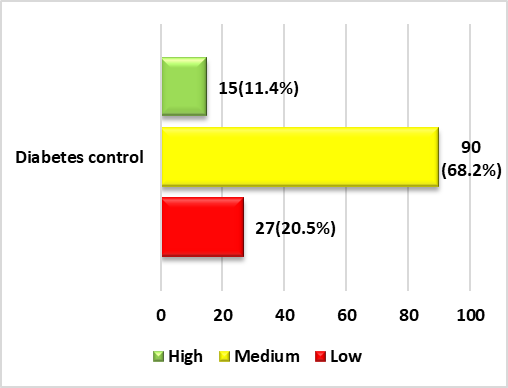
Figure 4. Quality
of life in terms of diabetes control among diabetic patients treated at a
hospital in northern Lima
In figure 4, we can see
that 11,4 % (n=159) of participants have a high quality of life in terms of
diabetes control, 68,2 % (n=90) h ve an average quality of life, and 20,5 %
(n=27) have a low quality of life.
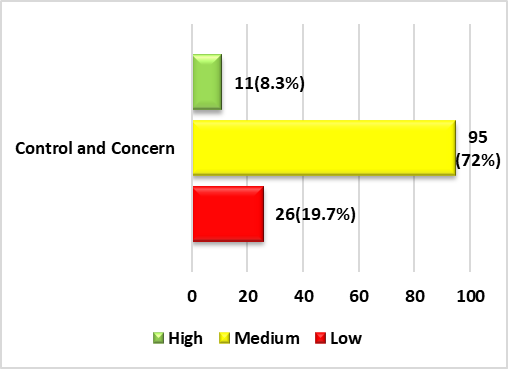
Figure 5. Quality
of life in terms of control and concern among diabetic patients treated at a
hospital in northern Lima
In figure 5, we can see
that 8,3 % (n=11) have a high quality of life in terms of control and concern,
72 % (n=95) have an average quality of life, and 19,7 % (n=26) have a low
quality of life.
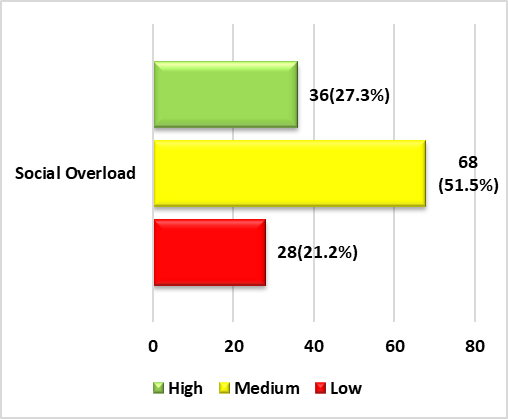
Figure 6. Quality
of life in terms of social burden among diabetic patients treated at a hospital
in northern Lima
Figure 6 shows that
27,3 % (n=36) of participants have a high quality of life with respect to their
social burden dimension, 51,5 % (n=68) have a medium quality of life, and 21,2
% (n=28) have a low quality of life.
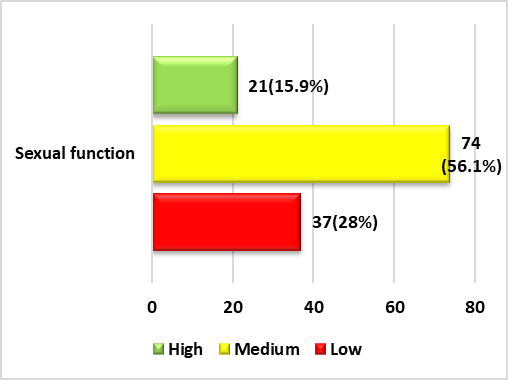
Figure 7. Quality
of life in terms of sexual function among diabetic patients treated at a
hospital in northern Lima
Figure 7 shows that
15,9 % (n=21) of participants have a high quality of life in terms of sexual
function, 56,1 % (n=74) have an average quality of life, and 28 % (n=37) have a
low quality of life.
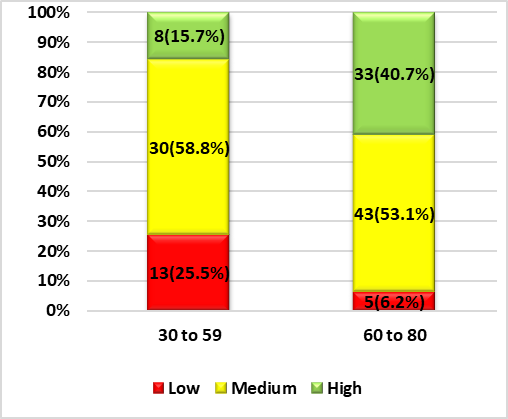
Figure 8. Quality
of life in relation to the ages of diabetic patients treated at a hospital in
northern Lima
In figure 8, we can see
that 15,7 % (n=8) of participants between the ages of 30 and 59 have a high
quality of life, 58,8 % (n=30) have an average quality of life, and 25,5 %
(n=13) have a low quality of life. and participants between the ages of 60 and
80, 40,7 % (n=33) have a high quality of life, 53,1 % (n=43) have an average
quality of life, and 6,2 % (n=5) have a low quality of life.
DISCUSSIONS
This study focused on
cardiovascular and metabolic diseases, with a view to promoting cardiovascular
risk prevention in diabetics and nursing care for diabetic patients.
In the results on
quality of life in diabetics, we observed that they have a measured quality of
life. We interpret this to mean that all diabetic patients, as they live with
the disease, tend to modify their lifestyle, where self-care will play an
important role for the diabetic person, where a healthy diet, exercise,
following the treatment correctly, and good family interaction will enable them
to maintain and improve their quality of life, minimizing the risks that their
disease can cause, and in turn allowing them to live a normal life by following
the advice of health professionals, who seek strategies to improve self-care in
diabetic patients, which fundamentally allows them to develop coping skills for
the disease, improving their physical, mental, and family behavior.
Although it is more
common in older people than in young people, as young people tend to be very
careless about their health, diabetes appears more easily due to high exposure
to glucose, where factors such as sugars, fat, and carbohydrates are factors
that are often associated with high blood pressure, high cholesterol, and
obesity, and these diseases are often significantly related to diabetes.
Therefore, the body, not being able to cope with such consumption, does not
usually adapt to the new situation, since, being a young organism, it does not
usually adapt quickly to the increase in glucose. Therefore, the risk of
developing diabetes is greater if healthy habits are not adopted to prevent
this disease from accompanying the person for the rest of their life.
The results of the
dimensions show that the diabetic people in the study have a quality of life in
relation to all dimensions. We can interpret this to mean that the changes made
by diabetic people often cause conflicts in their bodies, given that the activities
they used to do and the foods they used to eat and can no longer consume as a
result of the disease. Occasionally, the quality of life of people with
diabetes improves, as coping with the disease by correctly following the coping
strategies given by their healthcare professional allows them to maintain a
stable quality of life in the face of the disease they are suffering from.
CONCLUSIONS
It is concluded that motivational counseling should
be provided to people with diabetes on self-care to increase behavioral and
emotional levels.
It is concluded that talks should be given on
promoting a healthy lifestyle, aimed at people with diabetes mellitus.
BIBLIOGRAPHIC REFERENCES
1. D. Chipana, M.
Chipana, R. Villegas, B. Meneses, and H. Matta, “Type 2 diabetes risk and
physical activity in outpatients treated in health centers in a district of
north Lima, 2020,” Adv. Sci. Technol. Eng. Syst.,
vol. 5, no. 6, pp. 1651–1656, 2020, doi: 10.25046/aj0506196.
2. J. Santos et
al., “Qualidade de vida de pessoas com Diabetes Mellitus acompanhadas pela
Unidade Básica de Saúde,” Rev. Cubana Enferm., vol. 37, no. 1, pp. 1–14, 2021, https://orcid.org/0000-0002-3452-5759.
3. R. Tamornpark, S.
Utsaha, T. Apidechkul, D. Panklang, F. Yeemard, and P. Srichan, “Quality of
life and factors associated with a good quality of life among diabetes mellitus
patients in northern Thailand,” Health Qual. Life Outcomes, vol. 20, no. 81,
Dec. 2022, doi: 10.1186/s12955-022-01986-y.
4. B. Meneses, N.
Gonzalez, W. Alvarado, and J. Meneses, “Quality of life in patients with
diabetes mellitus treated in an outpatient clinic of a hospital in North Lima,”
Int. J. Adv. Appl. Sci., vol. 9, no. 5, pp. 1–8, 2022, doi:
10.21833/ijaas.2022.05.001.
5. M. Martins and M.
Rodrigues, “Diabetes: Patient Adhesion and the Role of the Family in this New
Reality,” Rev. Atenção à Saúde, vol. 17, no. 59, pp. 2359–4330, May 2019, doi:
10.13037/ras.vol17n59.5838.
6. J. Zavala, F. Mego,
S. Cornejo, B. Meneses, H. Solis, and L. Matta, “Quality of life in patients
with type 2 diabetes of the central hospital of the Peruvian Air Force, 2019,”
Adv. Sci. Technol. Eng. Syst., vol. 5, no. 6, pp. 1340–1344, 2020, doi:
10.25046/AJ0506160.
7. S. Moawd, “Quality
of Life in University Students with Diabetes Distress: Type 1 and Type 2 of
Diabetes Differences,” J. Diabetes Res., vol. 1, no. 1, pp. 1–7, 2022, doi:
10.1155/2022/1633448.
8. E. Beverly, R.
Rennie, E. Guseman, A. Rodgers, and A. Healy, “High Prevalence of Diabetes
Distress in a University Population,” J. Am. Osteopath. Assoc., vol. 119, no.
9, pp. 556–568, Sep. 2019, doi: 10.7556/jaoa.2019.099.
9. L. Fernández, A.
Rodríguez, A. Humberto, and A. Díaz, “Quality of Care for Type 2 Diabetic at
José Antonio Echeverría Polyclinic,” Rev. Finlay, vol. 9, no. 4, pp. 1–10,
2019, http://www.revfinlay.sld.cu/index.php/finlay/article/view/715.
10. K. Reyes et
al., “Calidad de vida en pacientes con Diabetes Mellitus tipo II, en Pachuca
Hidalgo,” Inst. Ciencias la salud Univ. Auton. del Estado Hidalgo, vol. 8, no.
15, pp. 1–6, 2019, https://repository.uaeh.edu.mx/revistas/index.php/ICSA/issue/archive.
11. H. Rezakhani, E.
Sobhi, and A. Habibi, “Determinants of Quality of Life among elderly Patients
with Type 2 Diabetes in Northwest of Iran: based on problem areas in diabetes,”
Front. Endocrinol. (Lausanne)., vol. 13, no. 1, pp. 1–8, Jul. 2022, doi:
10.3389/fendo.2022.924451.
12. C. Komaratat, N.
Auemaneekul, and W. Kittipichai, “Quality of life for Type II Diabetes Mellitus
patients in a Suburban tertiary Hospital in Thailand,” J. Heal. Res., vol. 35,
no. 1, pp. 3–14, Jan. 2021, doi: 10.1108/JHR-05-2019-0100.
13. I. Gálvez,
M. Cáceres, J. Guerrero, C. López, and N. Durán, “Calidad de vida relacionada
con la salud en pacientes con diabetes mellitus en una zona básica de salud,”
Enferm. Clin.,
vol. 31, no. 5, pp. 313–322, Sep. 2021, doi: 10.1016/j.enfcli.2021.03.001.
14. T. Gebremedhin, A.
Workicho, and D. Angaw, “Health-related quality of life and its associated
factors among adult patients with type II Diabetes attending Mizan Tepi
University Teaching Hospital, Southwest Ethiopia,” BMJ Open Diabetes Res. Care,
vol. 7, no. 1, p. e000577, Feb. 2019, doi: 10.1136/bmjdrc-2018-000577.
15. E. Vieira, F.
Stumpf, J. Carneiro, R. Pontarolo, and A. Wiens, “Evaluation of the application
of the diabetes quality of life questionnaire in patients with diabetes
mellitus,” Arch. Endocrinol. Metab., vol. 64, no. 1,
pp. 59–65, Jan. 2020, doi: 10.20945/2359-3997000000196.
16. B. Farías
and D. Bardales, “Conocimientos sobre Diabetes Mellitus tipo 2 y Adherencia al
tratamiento en pacientes del Hospital Reátegui, Piura, Perú,” ACTA MEDICA
Peru., vol. 38, no. 1, pp. 34–41, Apr. 2021, doi: 10.35663/amp.2021.381.1119.
17. C. Fernández
and P. Baptista, “Metodología de la Investigación.” p. 634, 2015. http://observatorio.epacartagena.gov.co/wp-content/uploads/2017/08/metodologia-de-la-investigacion-sexta-edicion.compressed.pdf.
18. J. Boyer and J.
Earp, “The Development of an Instrument for Assessing the Quality of Life of
People with Diabetes: Diabetes-39,” Med. Care,
vol. 35, no. 5, pp. 440–453, 1997, doi: 10.1097/00005650-199705000-00003.
19. J. López and
R. Rodríguez, “Adaptación y validación del instrumento de calidad de vida
Diabetes 39 en pacientes Mexicanos con diabetes mellitus tipo 2.,” Salud
Publica Mex., vol. 48, no. 3, pp. 200–211, 2006, doi:
10.1590/S0036-36342006000300004.
FINANCING
None.
CONFLICT OF INTEREST
Authors declare that
there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: David Hugo Bernedo-Moreira, Alfredo Giovanni
Lazo-Barreda, Paul Espiritu-Martinez, César Carbache Mora, Aaron Samuel Bracho
Mosquera.
Data
curation: David Hugo Bernedo-Moreira, Alfredo
Giovanni Lazo-Barreda, Paul Espiritu-Martinez, César Carbache Mora, Aaron
Samuel Bracho Mosquera.
Formal
analysis: David Hugo Bernedo-Moreira,
Alfredo Giovanni Lazo-Barreda, Paul
Espiritu-Martinez, César Carbache Mora, Aaron Samuel Bracho Mosquera.
Drafting
- original draft: David Hugo
Bernedo-Moreira, Alfredo Giovanni Lazo-Barreda, Paul
Espiritu-Martinez, César Carbache Mora, Aaron Samuel Bracho Mosquera.
Writing
- proofreading and editing: David Hugo
Bernedo-Moreira, Alfredo Giovanni Lazo-Barreda, Paul
Espiritu-Martinez, César Carbache Mora, Aaron Samuel Bracho Mosquera.